

Patients who have had strokes, head injuries, hydrocephalus, tumors, craniotomies, vascular issues, ruptured aneurysms, hemorrhages, hepatic encephalopathy and infections have reasons to have intracranial hypertension which means elevated ICP. As nurses, caring for critically ill patients, it’s essential we understand ICP, what it means for our patients and the nursing interventions to manage it. Understanding and recognizing elevated ICP is vital to preventing a terrible outcome.
The Monro-Kellie doctrine states that the cranium is a limited space that encompasses the brain tissue, blood and cerebral spinal fluid. Any increase in one of these components necessitates a change in the volume of another, now referred to as MK 1.0 “Any increase in the volume of one component must be compensated by a proportional reduction in another to maintain stable ICP” Rabelo (2021).
There have been advancements to the Monro-Kellie doctrine to add MK 2.0, 3.0 and 4.0. It is now understood that venous outflow from the brain can be impacted by external factors such as increased intrathoracic or intra-abdominal pressure or mechanical compression to the jugular veins. MK 2.0 states that venous occlusion or impaired outflow can independently increase ICP outside of arterial or CSF changes. MK 3.0 is yet a newer concept which states that with idiopathic intracranial hypertension and normal pressure hydrocephalus, the brain can undergo cerebral morphologic changes as well the skull can undergo remodeling. MK 4.0 underscores the importance of a multimodal approach to understanding cerebrovascular dynamics. Brasil (2025) explains:
“The core concept of MK 4.0 recognizes that in neuro emergencies such as traumatic brain injury (TBI), subarachnoid hemorrhage (SAH), and ischemic stroke per example, cerebrovascular autoregulation (CA), the glymphatic system (GS) and cerebral compensatory reserve are key determinants of ICP regulation and patient outcomes.”
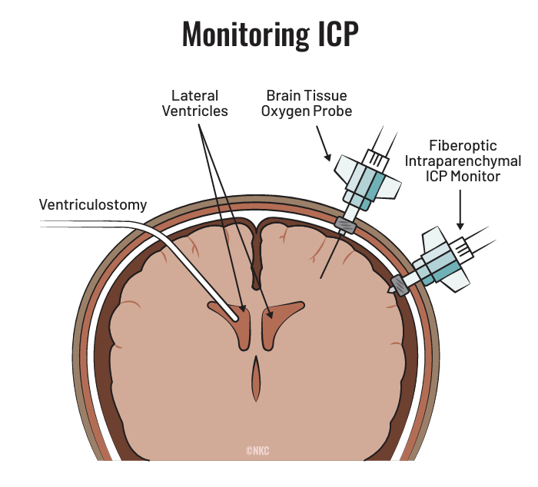
How to measure ICP:
- a probe/subarachnoid screw or “bolt”/Camino
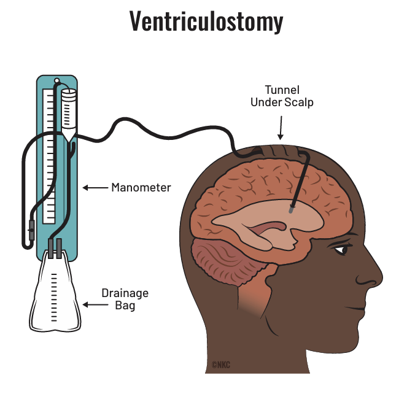
- transducing a ventriculostomy drain
Normal values:
- 0 – 15 mm Hg
Treatment is indicated if sustained > 20 – 25 mm Hg
Increased ICP leads to decreased cerebral perfusion which leads to ischemia, cell death and worsening edema!
Remember, May is National Stroke Awareness Month! If you want more information on recognizing strokes, treating them and preventing them, check out Nicole’s on demand online Stroke Review Bootcamp course or if you want to increase your neuro knowledge, consider taking Nicole’s on demand CCRN Review Course or grabbing her Critical Care Survival Guide!
References
Brasil, S., Patriota, G.C., Godoy, D.A. et al. Monro-Kellie 4.0: moving from intracranial pressure to intracranial dynamics. Crit Care 29, 229 (2025). https://doi.org/10.1186/s13054-025-05476-7
Rabelo NN, da Silva Brito J, da Silva JS, de Souza NB, Coelho G, Brasil S, Frigieri G. The historic evolution of intracranial pressure and cerebrospinal fluid pulse pressure concepts: two centuries of challenges. Surg Neurol Int. 2021;12:274.
Intracranial Pressure Monitoring: Background, Indications, Contraindications
Evaluation and management of elevated intracranial pressure in adults – UpToDate
Management of acute moderate and severe traumatic brain injury in adults – UpToDate



Add comment